Measurement of Ambient Ionizing Radiation Exposure in Operating Consoles of Radiation Modalities in Cancer Hospital NORIN Nawabshah, Pakistan
(This article belongs to the Section Radiology Nuclear Medicine and Medical Imaging (RNM))
Export Citations
Cite
Waqar, M. , Afridi, T. A. , Soomro, Q. , Abbasi, A. S. and Shahban, M. (2022). Measurement of Ambient Ionizing Radiation Exposure in Operating Consoles of Radiation Modalities in Cancer Hospital NORIN Nawabshah, Pakistan. Journal of Engineering Research and Sciences, 1(6), 7–12. https://doi.org/10.55708/js0106002
Muhammad Waqar, Touqir Ahmad Afridi, Quratulain Soomro, Abdul Salam Abbasi and Muhammad Shahban. "Measurement of Ambient Ionizing Radiation Exposure in Operating Consoles of Radiation Modalities in Cancer Hospital NORIN Nawabshah, Pakistan." Journal of Engineering Research and Sciences 1, no. 6 (June 2022): 7–12. https://doi.org/10.55708/js0106002
M. Waqar, T.A. Afridi, Q. Soomro, A.S. Abbasi and M. Shahban, "Measurement of Ambient Ionizing Radiation Exposure in Operating Consoles of Radiation Modalities in Cancer Hospital NORIN Nawabshah, Pakistan," Journal of Engineering Research and Sciences, vol. 1, no. 6, pp. 7–12, Jun. 2022, doi: 10.55708/js0106002.
Elevated exposure from background radiations and health hazards for radiation workers have recently grabbed the attention of researchers. This study targeted to measure the background radiation levels in the operating console areas radiation facilities of NORIN, Nawabshah Pakistan. Ten operating consoles of different treatment and diagnostic machines were surveyed using a calibrated RM1001-RD LAMSE radiation monitor for the period of one year periodically and AEDR was calculated using standard formulas. The organ doses were calculated using recommended occupancy and conversion factors. The highest point with increased AEDR was found to be the operating console of cobalt-60 teletherapy machine (0.876 ± 0.03 mSv/yr), while the lowest at the Digital Radiography operating console (0.730 ± 0.03 mSv/yr). The standard error ranged between 0.02-0.03 %. These findings affirm a statistically significant difference in T-test values at a level of significance of 5% (P<0.05). The testes received the maximum dose (0.718 mSv/yr) followed by bone-marrow (0.604 mSv/yr) at Co-60 Teletherapy operating console. Conclusion: Based on these results, it was deduced that radiation levels are well within the permissible radiation limit of 1.0 mSv/yr prescribed by the ICRP and hardly about 37% of UNSCEAR limit of 2.4 mSv/yr. Therefore, all radiation workers are radiologically safe in operating console areas because all radiation protection and regulatory protocols are strictly observed in the working environment. This study eliminates the undue anxiety about the hazardous nature of radiation in the radiation workers of cancer hospitals.
1. Introduction
Radiation has a multifaceted nature; it is beneficial as well as dangerous for living beings. We come across numerous types of radiation having different intensities in daily activities. The common hazards of radiation include cancer, cataract, genetic mutation, degradation of skeletal bones and blood cells. If imparted in enough quantity, radiation dose can cause death of an individual as reported by [1]. As far as the background radiation is concerned, the major contributors to background radiation are the materials used for construction. They also cause the transfer of radionuclides into the environment, enhancing the background radiation levels. Radon gas, formed in earth crust, is the most abundant culprit of natural background radiation in the environment. Uranium-238 yields 222Rn after radioactive decay, which has a half-life of 3.82 days [2]. It’s inhalation results in its absorption and penetration into the lung tissues. This absorption entails severe damage to lungs and also a mutation which consequently causes lung cancer [3]. Internationally recommended annual safe exposure limit is set by International Commission on Radiation Protection (ICRP) for Ionizing radiation. Its value by ICRP is 1mSv/yr for general public as reported by [4]. On the other hand, the United Nation Scientific Committee on the Effects of Atomic Radiations (UNSCEAR) set the effective dose rate limit of 2.4mSv/yr [5]. These safe limits are suggested for indoor facilities including research labs, offices, conference rooms, lecture halls, ete. Many studies have been reported previously which show that areas with increased ambient radiation are found in Kerele, India; Yangjiang, China; and Ramsar, Iran as in [6]; and in Asia as well. Highest levels of outdoor background radiation were reported in Malaysia and the highest indoor levels were reported in Hong Kong and Iran by [7].
Along with natural background radiation, man-made radiation sources are also there. Among these artificial radiation sources, X-Radiation serves as the largest contributor to the world population. The effects of radiation have been divided broadly into two categories: the stochastic effects and non-stochastic or deterministic effects (IAEA 2009) [8]. In a study consisting of 114 documented cases of cancer, it is shown that the technical and medical staff were affected mostly. In another documented case, 359 radiologist expired because of skin and bone cancer induced by radiation [9]. The harmful effects of high level ionizing radiation have been ascertained but there is an ongoing debate about whether its low levels are beneficial or not.
The Nuclear Medicine Oncology and Radiotherapy Institute Nawabshah (NORIN) is a comprehensive healthcare facility for diagnosis, treatment, and research of malignant tumours [10]. It was established with the objective to adopt the latest research methodologies for cancer management. Radiotherapy, Radiology and Nuclear medicine are the main departments of a cancer hospital where all radiation modalities are used for diagnoses and treatment [11]. Special suites are designed for these modalities in which radiation protection is made sure though all aspects. Wall thicknesses, mazes and doors are designed in such a way that there is no leakage radiation outside the suite. Operating consoles, from where the technician operates and controls the function of machine, are the areas which are designed in a special manner for monitoring the machines. The radiation protection protocols are implied in such a way that the operator is safe from the hazards of radiation inside the console during operation of modality [12].
2. Methods and Materials
NORIN cancer hospital Nawabshah is situated in the rural area of Sindh, Pakistan. On average, this centre facilitates about 400 cancer patients per week. The three core departments of this hospital are radiotherapy, nuclear medicine and radiology. Ten operating consoles of radiation modality suites were selected for this study including operating consoles of CT-Scanner, DEXA, Conventional Simulator, Brachytherapy, Co-60 Teletherapy, Mammography, X-Ray unit, Gamma Camera-I, Gamma Camera-II and Digital Radiography. The data was periodically collected over the span of one year and was analysed for calculation of AEDR.
The study was carried out by using RM1001-RD LAMSE survey meter calibrated from Secondary Standard Dosimetry Laboratory PINSTECH Islamabad as shown in Figure 2 . This model of survey meters is well-suited for the survey of background radiation in hospitals. The readings were taken during working hours with the workers performing their routine task. The equivalent dose readings were recorded in µSv/hr directly from the display screen of the radiation meter. The results were then converted into micro-Sievert per year (µSv/yr) and then finally converted to milli-Sievert per year (mSv/yr). An occupancy factor of 0.8 was used as recommended by the UNSCEAR (2000) [13]. The Annual Effective dose rate (AEDR) was calculated by using the following expressions.
$$\text{Annual Effective Dose Rate} \left( \frac{\mu Sv}{yr} \right) = X \left( \mu \frac{Sv}{hr} \right) \times T \times OF$$
$$\text{AEDR} \left( \frac{\mu Sv}{yr} \right) = X \left( \mu \frac{Sv}{hr} \right) \times 8760 \times 0.8 \times 10^{-3}$$
Where; X=hourly dose rate, T=total number of hours in a year (8760 hrs) and OF=occupancy factor (indoor = 0.8). Based on 24 hours a day and 365 days in a year; the number of hours in a year was 24 x 365 = 8760 hours [14]. AEDR is the total annual effective dose rate (mSv/yr).

Radiation doses to some body organs/tissues such as the lungs, ovaries, bone marrow, testes, kidneys, liver and whole body due to inhalation were computed using equation mentioned below.
$$\text{Organ Dose} \left( \frac{\mu Sv}{yr} \right) = \text{AEDR} \times CF$$
Where CF is the conversion factor of organ doses from air dose. The value of CF is 0.64 for the lungs, 0.69 for bone marrow, 0.58 for ovaries, 0.62 for kidneys, 0.82 for testes, 0.46 for liver and 0.68 for whole-body [15]. For the statistical analysis of the data, independent T-test on SPSS 17 statistical software (SPSS Inc. USA) [16] was used and values at a level of significance of 5% (P<0.05).
Table 1: Annual effective dose rate values (mSv/yr) with standard deviation at different operating console areas at NORIN
Consoles | Mean (µSv/hr) | Mean (mSv/yr) | AEDR (mSv/yr) | P-Value (P < 0.05) |
CT-scan | 0.112 | 0.9782 | 0.785 ± 0.03 | 0.020 |
DEXA | 0.110 | 0.913 | 0.771 ± 0.02 | 0.0101 |
Simulator | 0.110 | 0.963 | 0.772 ± 0.19 | 0.0019 |
Brachytherapy | 0.104 | 0.912 | 0.735 ± 0.03 | 0.0032 |
Teletherapy | 0.125 | 1.095 | 0.876 ± 0.03 | 0.0120 |
Mammography | 0.110 | 0.963 | 0.773 ± 0.03 | 0.0194 |
X-ray Unit | 0.113 | 0.985 | 0.788 ± 0.019 | 0.0044 |
Gamma Camera-I | 0.114 | 0.993 | 0.794 ± 0.024 | 0.0170 |
Gamma Camera-II | 0.109 | 0.956 | 0.765 ± 0.025 | 0.007 |
Digital Radiography | 0.104 | 0.922 | 0.730 ± 0.03 | 0.0107 |
3. Results and Discussion
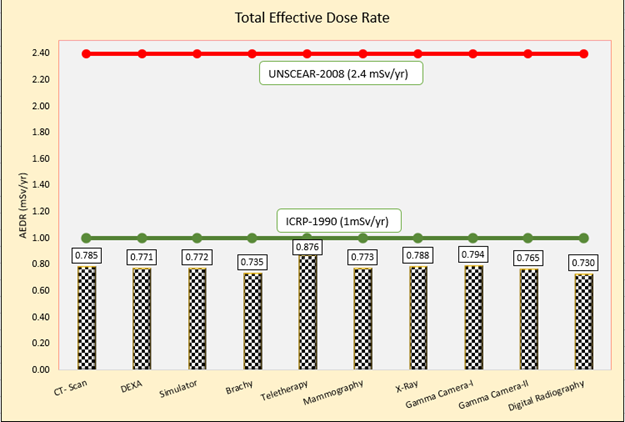
The 10 operating console of radiation modalities are required to assess the radiation risks associated with the scanning examinations and treatment of patients and worker in cancer Hospital Nawabshah, Pakistan. The results are presented in Tables 1 with mean values and AEDR (mSv/yr) and standard error with P values. Results are lower due to the strict following radiation protection protocols and all machines suites & operating Consoles rooms are prepared with PNRA & IAEA guidelines. Moreover, radiological burden of the hospital is within the permissible value of UNSCEAR in most of departments in hospital.
Figure 2 graphically represents the values of AEDR on ten selected operating console radiation suites and their comparison with globally accepted dose limits of ICRP and UNSCEAR. Each bar is associated with a suite and AEDR values are shown respectively. The maximum dose rate was shown at the console of Teletherapy machine (Cobalt-60) with value of 0.876 ± 0.03 mSv/yr. While the minimum does rate was observed in the operating console of the radiography room with AEDR of 0.730 ± 0.02 mSv/yr. It is clear from the graph that even the highest AEDR value (0.876 mSv/yr) is not more than that of annual dose limit of general public. While the annual background dose limit for a radiation worker is much higher with the value of 2.4 mSv/yr as shown the Figure 2 . Also, there is no area in the study where AEDR value goes above 1mSv/yr.
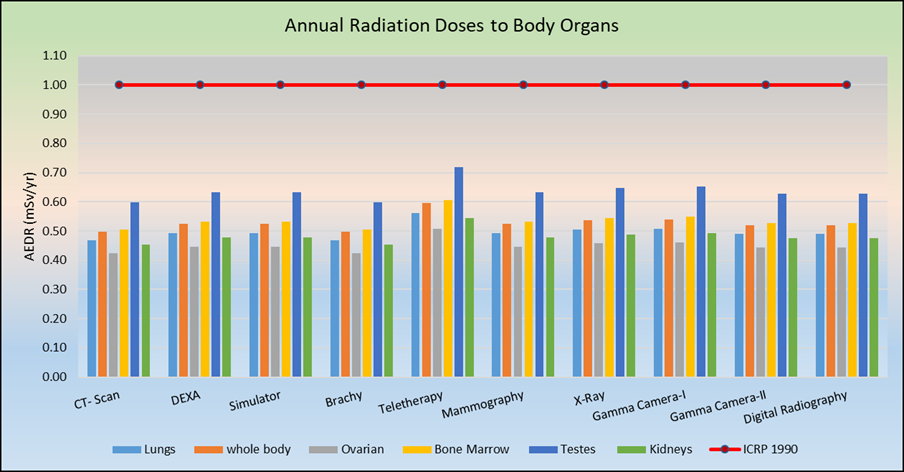
Organ/Tissue Specific radiation doses (lungs, ovaries, bone marrow, testes, kidneys, liver and whole body) to the radiation workers working in the operating consoles of various radiation modalities due to inhalation were computed and are graphically represented in Figure 3. It was observed that the most vulnerable organ prone to receiving maximum AEDR were testes with the highest mean AEDR of 0.718 mSv/yr at Cobalt-60 teletherapy console and minimum at CT-scan console. The lungs would receive at most (0.561 mSv/yr), whole body (0.596 mSv/yr), Ovaries (0.508 mSv/yr) Bone Marrow (0.604 mSv/yr) and kidneys (0.543 mSv/yr) recorded at Co-60 Teletherapy machine. All AEDRs were found well below the ICRP recommended limit of 01mSv/yr.
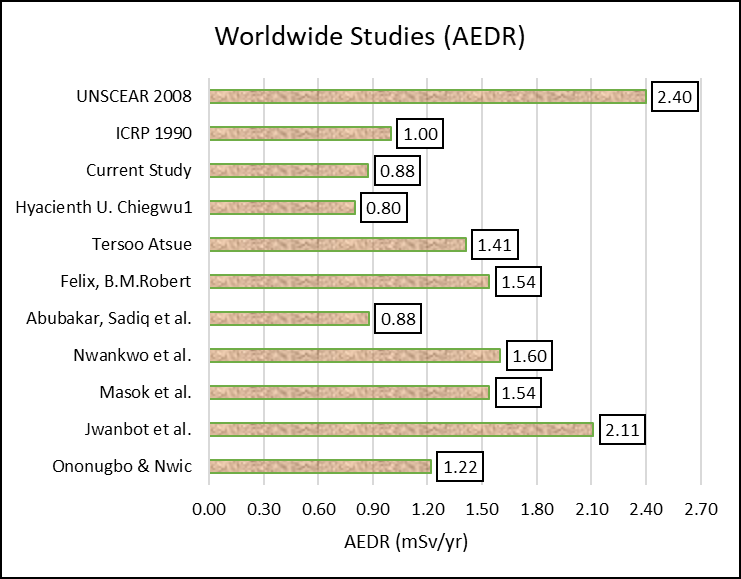
The Results of this study are lower compared with previous work. Some of the previous work is graphically summarized in Figure 4. In [17], the author reported 1.22 mSv/yr in a private medical diagnostic centre at Nigeria. A team of researchers found higher values of background ionizing radiation of 2.11 mSv/yr in some hospitals in Jos Plateau state, Nigeria [18]. Another study shows slightly higher values of 1.54 mSv/yr in the experimental labs of Plateau state university, Nigeria [2]. Pharmaceuticals facilities in Nigeria had dose rate of 1.60 mSv/yr [19]. In 2015, authors investigated the indoor background radiation levels at Plateau University Bookos and reported 1.54 mSv/yr [2]. Mean Indoor Annual Effective dose rate in the radiation labortries of Federal University KATSINA state, Nigeria documented 1.41 mSv/yr [9]. while the ICRP (1990) and UNSCEAR (2008) recommended annual dose level are 1.0 mSv/yr and 2.4 mSv/yr respectively [15]. However, a study carried out in Nigeria (2021) reported lower reading 0.80 mSv/yr than the results obtained from current study, while [20] reported the same (0.88 mSv/yr) ambient ionizing radiation level in Keffi General Hospital, Nigeria. This could be due to variations of equipment and office where no radiations are used.
The mean AEDR for the studied control rooms is comparable with the ICRP recommended annual limit of 1.0 mSv/yr for the general public but well below the UNSCEAR recommended world average value of 2.4 mSv/yr. This implies that the workers and people in those offices are radiologically safe.
Better knowledge about radiation due to exposure from patients is important for deciding on reasonable and appropriate precautions against unnecessary radiation exposure for radiation employees working in operating console and next-of-kin. Our results reaffirm that “undue anxiety among hospital staff with regard to exposure to radioactive patients must be placed in the proper perspective through education and training”. However, we observed that significant anxiety was still present. Perhaps particularly amongst staff not directly involved in hospital, but still in contact with the patients in other departments [21].
4. Conclusion
The findings of this study showed that there were no significant health hazards for radiation workers. The background exposure rate in different operating consoles of radiation modalities in this cancer hospital was well under the internationally recognized limits. Based on the aforementioned findings, it was deduced that radiation levels are within the permissible radiation limit as stipulated by the ICRP is 1.0 mSv/yr and UNSCEAR of 2.4 mSv/yr. The highest AEDR recorded in this study was in the console of Co-60 teletherapy machine which was 0.875 mSv/yr. Usually this area is considered as the area with the maximum ambient radiation levels in cancer hospitals and yet the AEDR calculated here was hardly 37% of the UNSCEAR recommended limit. This indicates that all radiation protection protocols are followed strictly as per regulatory guidelines. This study eliminates the undue anxiety about the hazardous nature of radiation in the radiation workers of cancer hospitals. Hence, all radiation workers in NORIN are radiologically safe in console areas and also, this facility does not elevate the radiation levels in the surrounding. Public health around the center is not on stake and there is no significant impact on the radiation burden of the environment.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgment
The authors are grateful to Mr. Sajad Hussain Langah, Mr. Junaid Faroque, Mr. Khadim Hussain and Mr. Murtaza Memon, Mr. Salam Baloch, Mr. Fayaz Hussain Langah, Ms. Saira Naz, Ms. Zulekhan and Ms. Rukhsana Kausar, Atomic Energy cancer hospital Nawabshah (AECH-NORIN) for their assistance in the collection of data.
- P. E. Ogola, W. M. Arika, D. W. Nyamai, K. O. Osano, and H. O. Rachuonyo, “Determination of background ionizing radiations in selected buildings in Nairobi County, Kenya,” J Nucl. Med. Radiat. Ther, vol. 7, no. 1, p. 289, 2016.
- F. B. Masok, R. R. Dawam, and E. W. Mangset, “Assessment of indoor and outdoor background radiation levels in Plateau State University Bokkos Jos, Nigeria,” 2015.
- C.-U. E. Yehuwdah, A. Martins, and H. O. Soibi, “Evaluation of indoor background ionizing radiation profile of a physics laboratory,” Facta Univ. Work. Living Environ. Prot., vol. 3, no. 1, pp. 1–8, 2006.
- J. T. Baraya, M. H. Sani, and M. Alhassan, “Assessment of indoor and outdoor background radiation levels at school of technology, Kano State Polytechnic, Kano State-Nigeria,” J. Appl. Sci. Environ. Manag., vol. 23, no. 3, pp. 569–574, 2019.
- U. N. S. C. on the E. of A. Radiation, “Sources and effects of ionizing radiation, ANNEX B, Exposures from natural radiation sources,” UNSCEAR 2000 REPORT, New York, vol. 1, pp. 97–99, 2000.
- S. S. Althoyaib and A. El-Taher, “The measurement of radon and radium concentrations in well water from Al-Jawaa, Saudi Arabia,” J Radioanal Nucl Chem, vol. 304, pp. 547–552, 2015.
- F. Alshahri, A. El-Taher, and A. E. A. Elzain, “Measurement of radon exhalation rate and annual effective dose from marine sediments, ras tanura, Saudi Arabia, using Cr-39 detectors,” Rom. J. Phys., vol. 64, p. 811, 2019.
- IAEA. and IAEA., Security of Radioactive Sources. International Atomic Energy Agency, 2009.
- T. Atsue and J. Adegboyega, “Assessment of the Ambient Background Radiation Levels at the Take-Off Campus of Federal University Dutsin-Ma, Katsina State-Nigeria,” FUDMA J. Sci. Maiden Ed., vol. 1, pp. 58–68, 2017.
- M. Waqar, M. Shahban, Q. Soomro, and M. N. Abro, “Institution-based assessment of cancer patients treated by external beam radiotherapy in the rural area of Sindh, Pakistan: Five years of data analysis,” Middle East J. Cancer, vol. 9, no. 3, pp. 217–222, 2018.
- M. Waqar, M. Shahban, Q. Soomro, T. A. Afridi, and N. Med, “Assessment of residual activities of Technetium-99m radiopharmaceuticals to plastic syringes in nuclear medicine scans : 1-year experience at NORIN,” vol. 12, no. 1, pp. 1–6.
- A. Razaq, M. Waqar, Q. Soomro, and M. A. Javed, “Evaluation of radiation workers occupational doses for newly established medical center NORIN Nawabshah in Pakistan,” J Med Phys Biophys, vol. 3, no. 1, pp. 61–65, 2016.
- N. Y. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) NY (United States), Sources and effects of ionizing radiation UNSCEAR 2000 report to the General Assembly, with scientific annexes Volume I: Sources. United Nations (UN): UN, 2000.
- U. Rilwan, A. U. Maisalatee, and M. Jafar, “Assessment of Indoor and Outdoor Radiation Exposure in Nasarawa General Hospital, Nasarawa State, Nigeria,” J. Radiat. Nucl. Appl. An Int. J., vol. 6, no. 3, pp. 245–249, 2021.
- H. U. Chiegwu et al., “Assessment of background ionizing radiation exposure levels in industrial buildings in Nnewi, Anambra State, Nigeria,” Int. J. Res. Med. Sci., vol. 10, no. 2, p. 305, 2022.
- M. Waqar, M. Shahban, Q. Soomro, and M. E. Khan, “Performance of Tc-99m Generators in Terms of Molybdenum Contents Measured in NORIN Nawabshah, Pakistan (5 years’ Experience),” Iran. J. Sci. Technol. Trans. A Sci., vol. 43, no. 1, pp. 285–289, 2019.
- C. P. Ononugbo and A. A. Nwii, “Indoor and Outdoor Effective doses from Background Ionizing Radiation in Private Medical Diagnostic Centers in Bori, Rivers State,” J. Environ. earth Sci., vol. 5, pp. 25–29, 2015.
- D. I. Jwanbot, M. M. Izam, G. G. Nyam, and I. S. Agada, “Evaluation of Indoor Background Ionizing Radiation Profile in Some Hospitals in Jos, Plateau State-Nigeria,” 2012.
- L. I. Nwankwo, D. F. Adeoti, and A. J. Folarin, “Ionizing radiation measurements and assay of corresponding dose rate around bottling and pharmaceutical facilities in Ilorin, Nigeria,” J. Sci. Technol., vol. 34, no. 2, pp. 84–92, 2014.
- A. Abubakar, A. A. Sadiq, M. G. Musa, J. Hassan, and D. F. Malgwi, “Assessment of indoor ionizing radiation profile in radiology department FMC Asaba Delta State Nigeria,” Internafional Organ. Scienfific Res. J. Dent. Med. Sci. 16 98, vol. 101, 2017.
- S. Harb, “Evaluation of radiation doses and radiation risk in Teaching Sohag Hospital, Egypt,” J. Nucl. Part. Phys., vol. 6, no. 4, pp. 88–93, 2016.
No related articles were found.