A Survey into Challenges and the Need for Heating Element Technology in Root Canal Procedures
(This article belongs to the Section Biomedical Engineering (BIE))
Export Citations
Cite
Pachpore, S. and Jadhav, P. (2022). A Survey into Challenges and the Need for Heating Element Technology in Root Canal Procedures. Journal of Engineering Research and Sciences, 1(12), 15–20. https://doi.org/10.55708/js0112003
Swanand Pachpore and Pradeep Jadhav. "A Survey into Challenges and the Need for Heating Element Technology in Root Canal Procedures." Journal of Engineering Research and Sciences 1, no. 12 (December 2022): 15–20. https://doi.org/10.55708/js0112003
S. Pachpore and P. Jadhav, "A Survey into Challenges and the Need for Heating Element Technology in Root Canal Procedures," Journal of Engineering Research and Sciences, vol. 1, no. 12, pp. 15–20, Dec. 2022, doi: 10.55708/js0112003.
Root Canal Treatment (RCT) is one of the most common endodontic clinical procedures performed in the field of dentistry amounting to almost 25 million performed every year. It is thus essential for endodontists to ensure best practices. However, through a recent survey, it has been observed endodontists resort to supplemental methods and protocols during procedures due to the scarcity of precision devices in the market. This not only compromises sound practices but also elevates the risk of operational failures & additional infections at the cost of the patient. Despite this deviation, the survey further highlights that touch and heat devices offer better stability, precision, and safety. This paper sets out to explore the ongoing challenges faced by endodontists in this field particularly in the methods to cut Gutta-percha and seal the canal and establish the need for heating element technology in such procedures.
1. Introductsion
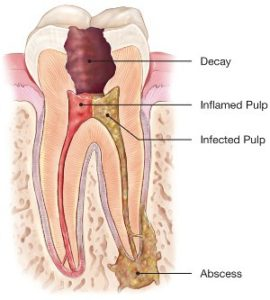
Root Canal Treatment (RCT) is used to extirpate a damaged or infected tooth pulp and clean and seal the interior of the tooth with gutta-percha to avoid further spread of infection [1]. The pulp of the tooth is a soft chamber within the tooth comprising nerves and blood vessels. The nerve endings are located near the root of the tooth and canals travel from the root tip to the tooth chamber. The tooth pulp gets affected and infected due to deep decay, multiple repeated dental procedures, large fillings, a crack in the tooth, or trauma to the face.
Infections due to deep cavities are one of the most common reasons leading to infections. When the pulp gets infected, a chemical breakdown occurs, and it becomes a site harvesting exponential bacterial growth [2]. A prolonged effect of increasing bacterial growth and the decomposing pulp will lead to pus formation. In the dental field, this process can be referred to as the formation of an abscessed tooth. The pus pocket or abscess is primarily categorized into a periapical abscess which forms at the tip of the tooth’s root and a periodontal abscess that affects the bone next to your tooth. This abscess formation can lead to the following issues-
- Spread of infection and swelling to other tooth, gum area and in severe but rare cases also affecting cheeks.
- Loss of bone around the tip of the root
- Generation of a hole cutting straight through the tooth and gums leading to a draining problem and increasing direct exposure to vital internal systems .
Thus, treating it as early as possible to avoid any further implications is of paramount importance. Endodontists provide RCT to the patients. However, due to ongoing challenges in the treatment procedures especially in the gutta percha cutting – sealing phase has probably made endodontists resort to unsafe practices which can be hazardous to the patient. We thus seek to assess and address the issues faced specifically in the gutta percha cutting sealing phase by doing a survey on ongoing challenges and get valuable inputs from endodontists. Based on the survey results we also seek to establish a need or a proposed methodology to overcome the difficulties faced in this profession [3].
2. Literature Review
2.1. Root Canal Treatment Procedure
In the RCT procedure the endodontist first proceeds to take an X-ray to assess the structure of root canals and determine any other affected area including infections on the adjacent bone. While performing the endodontist uses anesthesia to numb the surrounding area and places a sheet of rubber – rubber dam to avoid flow of saliva. A hole is then drilled through the tooth or through the existing cavity exposing the pulp and the infection as shown in Figure 1. All residual pulp is then removed. Continuous water treatment ensures remaining debris is removed. The endodontist then cleans the canal track using files, scraping the walls clean.
In presence of other internal infections, the endodontist provides treatment and may decide to seal the canal later. In such a case the tooth is filled with a temporary filling. In other cases, the endodontist seals the canals directly. This is done using a sealer and cones of a rubber compound gutta percha. These cones are tapered and are available in varied sizes to fit into the canal structure. Different techniques are used for filling in the Gutta percha cones and are outlined below.
Gutta-percha is a natural latex and is obtained from Palaquium Gutta and several other trees of East Asia. Based on their manufacturing process gutta-percha can be classified in two distinct forms (α and β) which can be interchangeable. During the manufacturing process, if the cooling is done rapidly, it results into the ‘β’ form which is the most commercially available form, whereas if it is cooled slowly, less than 0.5°C per hour, α form is produced. Typical properties of α include sticky, lower viscosity, fluid while β form is solid, compactible, has higher viscosity and can be elongated. Following are the various techniques of sealing and filling the canal with Gutta percha [4].
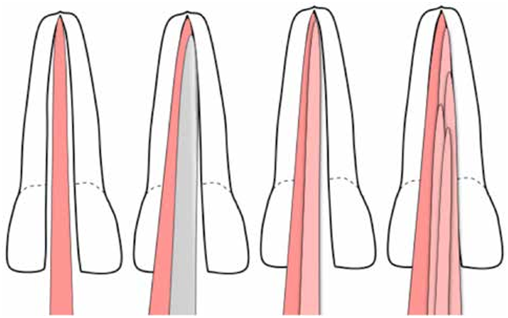
2.1.1. Lateral compaction of gutta-percha
In this particular technique, gutta percha cones are compacted laterally one over the other against the canal walls as shown in Figure 2. This technique has two subtypes – cold compaction and warm compaction. The cold lateral compaction comprises of arranging the gutta percha cones and filling the canal. Though it offers advantages such as simplicity, no additional cost, or specific instruments its disadvantages include risking formation of air gaps or voids and requires high precision. Additionally, gutta-percha placement is key in this technique to avoid inadequate filling.
The warm compaction method seeks to overcome these limitations by applying heat to the gutta percha. This is done usually using a heat carrier electrical device supplying constant heat to the tip. The soft gutta percha will provide better flow and result in a dense root filling. The cones are placed in a similar fashion to the cold compaction technique and then are pressed with a heated tip to provide better seal. Additionally, it will result in better flow through the root canal complexities. These specific instruments have a sharp tip for lateral compaction, and a blunt plugger tip for limited vertical compaction of the softened gutta-percha.
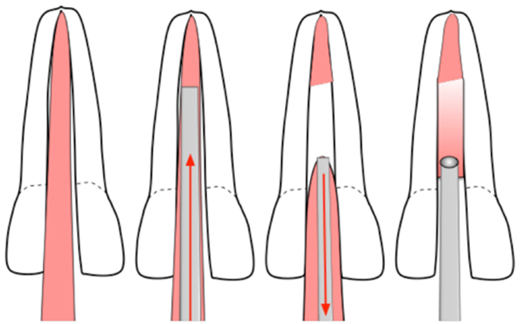
2.1.2 Vertical compaction of gutta-percha
This technique is similar to the heated lateral compaction only differing in the compaction axis. The soft gutta percha is pressed down vertically and the cones are added over the other to complete the filling and eventually obturate. As shown through Figure 3 gutta-percha cone is placed in the canal. The heated device tip then melts the gutta-percha providing fluid flow though the canal and with slight pressure the lower part of the canal is sealed. More cones are now added above the sealed portion and the process is repeated until the canal is filled [7].
In both methods heat and touch devices are used, the tip dimensions however differ in both techniques, but usually different tips can be attached to a single device based on application. Heated gutta-percha flow in both lateral and vertical compaction techniques provide the best sealing for canals. Vertical compaction method delivers the best results with very high accuracy however is used in rare cases as it is time consuming and takes time to be mastered [8]. It is not as widely used as lateral heated compaction as the latter is more feasible and easier to use. This method is useful in situations such as internal resorption, C- shaped canals, or canals with fin and webs.
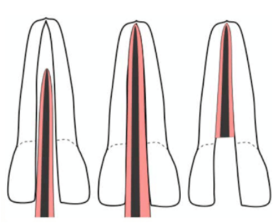
2.2. Gutta-Percha heated carriers
This method uses alpha-phase gutta-percha which gets attached around a rigid plastic heated carrier. It is placed directly in the canal and excess material is removed. The carrier and gutta percha once placed remain in the canal as shown in Figure 4. The carrier functions as a heated support structure. The softened gutta-percha then flows through the canal sealing it off completely. This technique however requires cleaning and canal shaping precision. The carrier’s structure and canal structure must match perfectly for a good fit. An irregular fit can cause problems such as formation of gaps between walls and the sealant [7].
2.2.1. Single gutta-percha
This technique utilizes the concept of custom fitting based on canal geometry. However, each individual may have unique structures, and the feasibility of this method is hence limited. A single gutta percha matching the structure of canal is used and in a single movement it is fitted in the canal. This method is usually not recommended [10].
2.2.2. Thematic compaction of gutta-percha
This method uses the principle of friction. A device having blades is used to compact and soften the gutta percha using frictional heat. It then drives the gutta percha deep into the canal. This technique however requires very high precision and practice to master. Additionally, low control has made this method unfit for practice as compared to other techniques.
2.2.3. Injectable gutta-percha
This is a developing technique focusing on directly injecting soft gutta – percha or sealant using obturation device. This technique however is not as effective. Each complex and deep canal structure would require a unique custom obturation tip to ensure complete flow, reach and sealing. Moreover, air gaps can be created if the device obturation tip falls short of the depth of the canal. These limitations make the technique less viable [11].
The heated lateral compaction technique is the most widely used technique for obturation although in some cases vertical heated compaction may also be used. The basic principle behind achieving this is to provide a constant heat supply through a narrow tip. The final step of the RCT procedure may include providing restoration of tooth. This is done to provide protection and avoid breaking [4]. It can be done through crown fitting, crown, and post. Thus, heat and touch devices form an integral part of the RCT. We hence seek to explore the available devices and challenges faced by endodontists in usage of such devices to ensure maximum accuracy [12].
2.3. Current methods & devices to cut and seal Gutta Percha
We now investigate the current available devices or methods used, and their features. As clearly indicated in Table 1 Sybron Endo outweighs all other devices/ techniques in use currently
Table 1: Methods and devices used
Method/ Device | Principle | Positive Aspects | Negative Aspects |
Direct Flame Usage | Heat slender rod directly on flame | Cheap | No accuracy, fire hazard, no constant heat supply. |
Woodpecker Touch and Heat[1] | Electric Heating | Handheld, suited for vertical compaction, 4temperature settings | Tip quality mediocre, Costly. |
Sybron Endo Touch and Heat 5004[2] | Electric Heating | High precision, most trusted, Variable heating, Ease of use & convenience, Variable tip size facilitating both compaction techniques, | Costly, No longer manufactured |
Napple GP Cutter | Electric Heating | Handheld offering high mobility and operability, cheap, | Tips are not usually made of high quality or geometry to suit compaction. Life expectancy is low. |
Gutta Cut (VDW GmbH, Endodontic Synergy) Germany. | Electric Heating | Induction charging unit + 4 tips, rechargeable, Ni-Cd battery | Low quality tips, low life expectancy 80 cuts per battery charge. |
3. Survey Results
We proceed to start with a questionnaire survey relating to challenges faced in the Gutta – Percha cutting and sealing phase of the RCT, advantages of touch and heat devices & the methods used currently. We try to infer the reasons behind the deviations from safe practices using this survey. Thus, our primary focus would be to find endodontists not using touch and heat devices despite having practiced or learnt about it earlier. With consultation of endodontists, we estimate minimum required sample size (n) to be 43 assuming a 95% confidence level, margin error (δ) 0.15 and proportion outcome (ϕ) 0.5.
$$n = \left( \frac{1.96}{\delta} \right)^2 \phi (1 – \phi)$$
The survey was conducted through more than fifty endodontists majorly across Pune Municipality region, and across India. Detailed analysis of the results can be found in the next section.
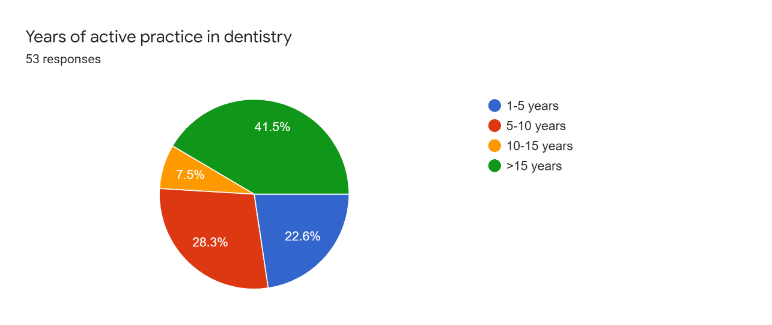
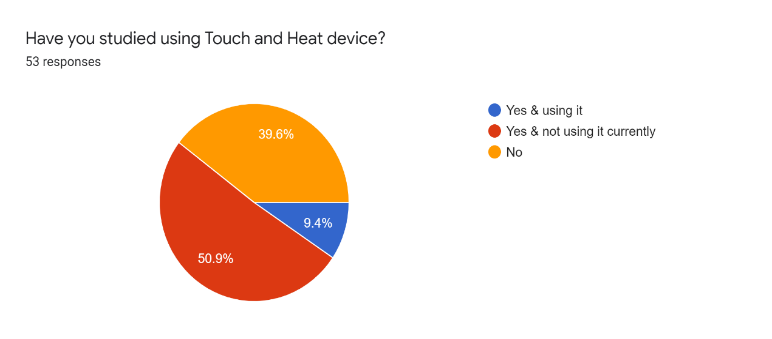
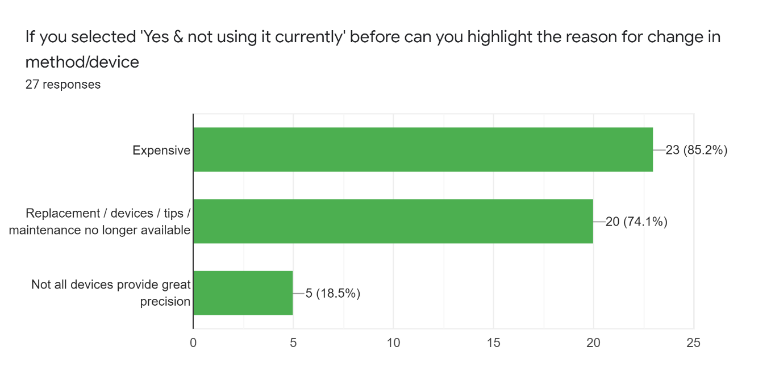
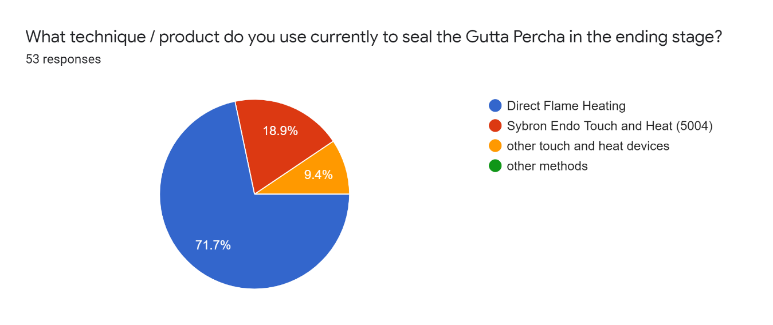
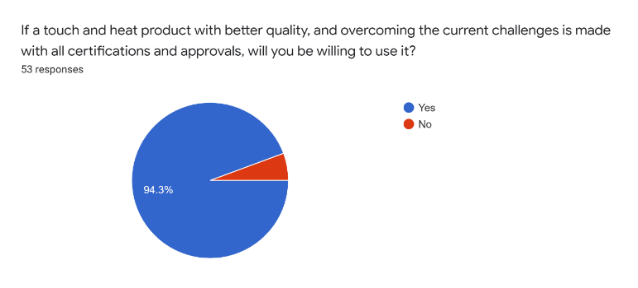
Table 2: Responses to new techniques and used techniques by practitioners
Any new techniques coming up for the same purpose / have you used different techniques apart from your current technique? |
Heated root filling material (Injectable Gutta-Percha) |
Cold Flowable Gutta-Percha (Research Stage) |
Table 3 : Responses advantages of techniques under use
How does your current technique differ from touch and heat devices? (Advantages) |
I) Sybron and other Touch and Heat Devices |
Easy to heat and cut the gutta percha |
User friendly, highly accurate (Sybron) |
Less time consuming, convenient |
Better flow and sealing of Gutta-Percha |
Continuous heat flow ensures good compaction |
I) Direct flame Heating |
Economical, Quick |
Effective, Fast, minimal maintenance |
Requires practice to attain precision. |
Table 4: Responses Disadvantages of techniques under use
How does your current technique differ from touch and heat devices? (Disadvantages) |
I) Sybron and other Touch and Heat Devices |
Costly, high maintenance |
Irreplaceable parts if device malfunctions |
Sybron has stopped manufacturing and other devices don’t offer similar accuracy. |
II) Direct Flame Heating |
Lifting of Gutta-Percha Points during procedure |
Poor seal and flow, less accurate |
Complex structures cannot be easily accessed. |
Cannot reach Tertiary roots |
Not patient friendly, can cause burns and other injuries |
4. Analysis
It is observed from Figure 5 that out of the survey population 39.6% have not studied using touch and heat devices and resort to direct flame heating and it can also be seen 41.5% have more than 15 years of practical experience. It was found that the theoretical aspects of such touch and heat methods were covered in the dentistry curriculum much recently, thus possibly explaining usage of the direct flame heating methods. However, it can also be observed through Table IV that this method has low accuracy and poses as a hazard if not practiced with precision. From Figure 10 it can be inferred that if touch and heat devices are made with lower costs, and ease of usability, this population bracket is willing to switch to a much safer and accurate method.
On the other hand, 60.4% of the population are familiar with the usage of touch and heat devices, but figure 1.7 reveals that only 9.4% use such devices for RCT implying only 15.56% of this population bracket is willing to practice with these devices. It can be clearly observed from Table III that the advantages of touch and heat devices especially Sybron Endo 5004, clearly outweigh those of the direct flame heating in terms of safety & precision. Touch and heat devices further allow better flow of Gutta Percha through canal leading to better sealing. These devices also facilitate reaching into complex canal structures and tertiary roots. The table IV also highlights numerous disadvantages of the direct heating technique like possible burning of lips/cheeks and non- stable heat flow. Thus, it is evident from these results that touch, and heat devices are safer and highly accurate and direct heating method although cheap, can be hazardous to the patient. Yet only 15.56% of this population bracket chooses to practice said technique.
Figure 8 tries to explore the possible reasons behind endodontists deviating from this technique. 85.2% of the respondents cited cost as one of the reasons while 74.1% cited unavailability of device maintenance, parts, or replacement. Endodontists resort to usage of direct flame heating whenever the touch and heat device malfunctions. A touch, and heat device Sybron Endo, with its features listed in table I has the highest market share in this segment. Its positive features outweigh all other touch and heat devices. However, it was noted that Sybron has currently shut down its operations across India and devices and other accessories if available are imported at heavy costs.
It can be inferred from Figure 9 that Sybron Endo is the most used and trusted device during RCT procedures and thus its scarcity has impacted its practice. Unavailability of device maintenance and replacement parts makes this device unviable. Furthermore Figure 8 and Figure 9 also conveys that despite a broad market endodontist do not prefer to use other devices citing quality concerns. Other touch and heat devices as also highlighted in table I do not seem to match either the quality or the precision of the Sybron device. A combined effect of scarcity and unreliable products in the same segment has potentially caused endodontists to shift to unsafe practices.
Table II highlights 2 upcoming techniques cold flowable gutta-percha and injectable gutta-percha. The first technique is in its nascent stage while the second technique faces issues as highlighted in section 2.1.6. Thus, any significant developments to improve quality of other touch and heat devices to match Sybron endo has not been possible yet. This possibly explains why endodontists are currently resorting to direct flame heating technique which is a cheap substitute but raises operational risks. Figure 10 and Table III conclude that practitioners would prefer to use touch and heat devices over direct flame heating technique which in turn can ensure safe practices. Thus, it is evident that there is a need to develop highly accurate touch and heat approaches in this field to assist endodontists for better accuracy and safety.
5. Conclusion
Touch and heat devices offer better stability, reliability and safety compared to direct flame heating technique. They are more accurate and can reach complex structures with ease. They also have stable heat flow ensuring proper cutting and sealing. Although costs for touch and heat devices in the market are substantial. Additionally direct flame heating technique poses dangers to the patient such as burns.
The survey results showed that unavailability of touch and heat devices in particular Sybron Endo 5004 or parts for replacement and other unreliable market players have made majority of the endodontists move to direct flame heating technique as a cheaper alternative. Others cite concerns over precision and functionality of other heat and touch devices as a reason of shift to direct flame heating technique.
Having high quality touch and heat devices for the purpose of compaction and Gutta Percha cutting is a necessity to ensure safe, accurate practices and endodontists would prefer to use such devices provided they get necessary certifications from the medical board.
Conflict of Interest
The authors declare no conflict of interest.
- S. S. Pachpore, P. V. Jadhav, R. R. Ghorpade, “Analyzing Relation of Canal Operating Force and Canal Curvature in RCT: A Mathematical Overview”, Materials Today: Proceedings, vol. 47, no. xxxx, pp. 5690–5696, 2021, doi:10.1016/j.matpr.2021.03.746.
- B. A. Alim, Y. Garip Berker, “Evaluation of different root canal filling techniques in severely curved canals by micro-computed tomography”, Saudi Dental Journal, vol. 32, no. 4, pp. 200–205, 2020, doi:10.1016/j.sdentj.2019.08.009.
- A. Galande et al., “Investigation and assessment for specific volume of Gutta-Percha as a biomaterial in RCT”, Materials Today: Proceedings, 2022, doi:https://doi.org/10.1016/j.matpr.2022.08.499.
- M. R. Hameed, A. H. Ali, M. M. Rashad, “Obturation of lateral canals by a new reciprocating spreader and a conventional finger spreader by lateral condensation technique: In vitro comparative study”, World Journal of Dentistry, vol. 9, no. 4, pp. 265–269, 2018, doi:10.5005/JP-JOURNALS-10015-1546.
- P. B. Borade et al., “Root Canal Filling Process Enhancement in Simulated Dental Block Using Root Canal Filling Process Enhancement in Simulated Dental Block Using Static Analysis”no. November, 2020.
- C. M. Friedman et al., “Composition and Mechanical Properties of Gutta-Percha Endodontic Points”, Journal of Dental Research, vol. 54, no. 5, pp. 921–925, 1975, doi:10.1177/00220345750540052901.
- R. R. Ghorpade, K. Sundaram, H. Vivek, “Thermal & Stress Analysis of Gutta Percha in Simulated Root Canal using finite Element Analysis”, International Journal of Mechanical and Production Engineering Research and Development, vol. 2, no. 4, pp. 19–30, 2012.
- H. F. Smith CS, Setchell DJ, “Factors influencing the success of root canal therapy: A five year retrospective study. Int. Endodo. J. 1993;26:321- 333.”, International Endodontic Journal, vol. 26, no. 1961, pp. 321–333, 1993.
- F. R. Tay et al., “Geometric Factors Affecting Dentin Bonding in Root Canals : A Theoretical Modeling Approach”vol. 31, no. 8, 2005.
- T. Bogoni, R. Scarparo, M. Pinho, “A virtual reality simulator for training endodontics procedures using manual files”, 2015 IEEE Symposium on 3D User Interfaces, 3DUI 2015 – Proceedings, pp. 39–42, 2015, doi:10.1109/3DUI.2015.7131724.
- JLC Electromet, “Nickel-Chromium: Heating Element & Resistance Alloys”no. March, pp. 2–3, 2016.
- O. Article, “Comparison of Obturation Density Using Nickel Titanium and Stainless Steel Spreaders by Lateral Compaction Technique”pp. 54–59, 2012.
No related articles were found.